Survey Aims
The Malaria Behavior Survey (MBS) aims to:
- Provide a better understanding of the socio-demographic and ideational characteristics associated with malaria-related behavioral outcomes at the zonal level in a given country, and
- Determine the appropriate focus of programmatic activities designed to improve malaria-related behavioral outcomes.
Conceptual Model
The MBS is intended to inform malaria social and behavior change programs by measuring several social science indicators about malaria prevention and care-seeking behaviors. Theories of behavior change rely on social science concepts to explain what influences people’s behaviors. These theories are derived from scientific observations and studies of human behaviors. Because it studying every behavior in every context is not possible, theories provide a framework to build conceptual models that guide formative research.
The conceptual model behind the questions in the MBS is the ideation model of behavior change, which combines the theory of diffusion of innovations and the social network theory and refers to how ideas, ways of thinking, and behaviors are developed and disseminated to others through communication and social interaction. Ideation can be used to identify the psychosocial factors associated with behaviors, determine the contextual and environmental conditions that facilitate behaviors, and provide guidance about which SBC and service delivery strategies should be emphasized to influence behaviors. Understanding the drivers of malaria-related behavior helps countries and program planners determine the appropriate focus of national and sub-national social and behavior change (SBC) programmatic activities to reduce the burden of malaria. Ideation model constructs measured by the MBS are defined below:
Study Design
Being a population-based survey, the MBS in every country uses a different sampling frame and is usually split into two or more survey zones that combine several subnational administrative units (e.g., regions, districts). That decision is made with country stakeholders and informed by key considerations for establishing groupings of areas that are considered important by the stakeholders, such as malaria transmission patterns and major ethnic/linguistic groups. Each country MBS report will detail the specific geography represented by the survey zones.
The MBS is a quantitative, cross-sectional survey of randomly selected household heads, women, and men. Participants are interviewed using theory-driven, structured questionnaires and are selected through a multi-stage, cluster random sampling technique that involves i) selection of enumeration areas based on probability proportional to the population size, ii) a random selection of eligible households within enumeration areas, and iii) selection of all eligible individuals within the randomly selected households.
A household is eligible for participation in the MBS if there are at least one female aged 15-49 years of age residing in the household. A woman is eligible for participation if she is between 15-49 years of age at the time of the survey, with parental consent required for respondents under the age of 18. All eligible women in a selected household are invited to participate. In one-third of the selected households, the female respondent’s male partner or spouse is also eligible to participate if he is between 18 and 59 years of age.
The MBS is designed to be conducted during or very shortly after the rainy season in malaria control areas with moderate to high malaria prevalence. An adaptation of the MBS for implementation in malaria elimination areas with lower malaria prevalence is available (9).
Sample Size Determination
The sample size is calculated to provide point estimates of malaria-related outcome indicators to a specified level of statistical certainty. The following formula is applied to estimate the required sample size:
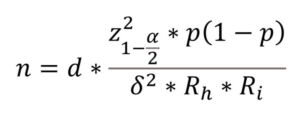
Where:
n is the required sample of individuals (e.g., women).
Z is the Z value (assumed that Z=1.96) corresponding to the desired confidence level (assumed 95% confidence level).
d is the design effect due to departure from simple random sampling (assumed to be 2.5).
p is the estimated (expected) outcome indicator based on existing data. For outcomes that were not available in publicly available data sets (e.g., Malaria Indicator Survey [MIS] or the Multiple Indicator Cluster Survey [MICS]), a proportion of 50% (p=0.5) is assumed for maximum variability.
δ is the desired margin of error. Various sample sizes are derived with δ=5%.
Rh is the expected response rate for households. 90% is assumed for this parameter.
Ri is the expected response rate for women in selected households. 95% is assumed for this parameter.
Determining the required sample size for the MBS is based on several factors, including:
- The geographic level at which the study will be able to make inferences.
- Prevalence of behavioral or ideational indicators that the program plans to measure. These indicators should be relevant to the country’s Malaria SBC strategy. In most cases, these will draw from indicators available in MICS or MIS studies.
- Type of sample (i.e., whether a one-time or repeated cross-sectional design).
Sampling in Low Transmission Areas
Malaria transmission patterns are different in low transmission settings, potentially resulting in greater clustering of cases. The low transmission MBS provides an opportunity to customize the sampling approach and questionnaires to help malaria programs target interventions and support SBC activities and messaging more effectively.
Areas with low transmission, defined as annual parasite incidence (API) of 100-250 cases per 1000 population and very low transmission (<100 API per 1000 population), are distinct from other transmission contexts in several important ways. This includes:
- Where cases are distributed: low transmission contexts often experience increased focalization of malaria cases and reservoirs in certain geographic areas. While the cases may be geographically focalized, they may be in hard-to-reach locations.
- Who is most likely to be infected: there is often increased case focalization in adults, particularly men. Occupation-based exposure and risk of imported cases from population movement and seasonal migration are also key considerations. These populations may be hard to reach due to the nature of their work, for example, in illegal hunting or logging.
- What interventions are deployed: while core interventions remain important, several additional interventions may be implemented by malaria programs in lower transmission settings to target malaria parasites and vectors. Approaches need to be tailored, underscoring the importance of context-specific data to inform SBC interventions.
Please see the Low Transmission MBS Implementation Guidelines for more information.
Questionnaire Administration
The household questionnaires explore household characteristics, ownership of assets, and a roster of all bed nets in the house. The MBS uses a nearly identical methodology to measure ITN access and use as the MIS and DHS, and the same net roster questions employed by the MIS. Other indicators in common with the MIS include children with fever two weeks before the survey, prompt and appropriate care-seeking, average number of ANC visits by pregnant women in the two years before the survey, and average number of IPTp doses by pregnant women in the two years before the survey.
Both women’s and men’s questionnaires include modules assessing net use frequency, net care practices, perceptions of health services, and ideational factors, including knowledge, perceived severity, perceived vulnerability, perceived response efficacy, attitudes, perceived self-efficacy, norms, social interactions, and influence, related to malaria behaviors, as well as exposure to malaria-related communication interventions.
The questionnaire for women explores antenatal care and receipt of IPTp among those who had a live birth within the past two years, seeking appropriate care for the youngest child under five years of age (index child) who most recently had a fever in the past two weeks. The questionnaire for men includes questions related to their contribution or support to their partner for various malaria or behavioral-related outcomes and attitudes and other perceptions. Questionnaires are administered in the relevant local languages using electronic data collection software.
Analysis
In addition to descriptive analysis, bivariate, and multivariate analytic methods are used to assess the relationships between sociodemographic characteristics, ideational factors, and the outcomes of interest. Bivariate analyses examine how each potential correlate is associated with dependent outcomes. Using the variables that were significant from this step as well as variables identified from a priori knowledge, multivariate regression models are used to detect the association with the dependent variables after controlling for potential confounding factors. The dependent variable is the malaria-related behavior or outcome of interest, and independent variables include region, urban/rural residence, education level, age, marital status, religion, household size, wealth quintile, media exposure, and ideational variables (such as perceived severity, perceived susceptibility, perceived self-efficacy, perceived response efficacy, attitudes, knowledge, etc.).
For ideational factors that are assessed based on several items, a composite variable is created by developing a score on the items intended to measure that factor for each respondent. The score is then split at zero to denote positive versus negative ideation. In cases where the average score is very high and splitting at zero would result in most respondents (e.g., 90% or more) being classified as having positive ideation, the score can be split at the highest value to denote higher versus lower levels of ideation on that factor. The composite variable is used in the multivariable regression model.
Ethical Approval
All MBS surveys conducted by Breakthrough ACTION receive Institutional Review Board (IRB) approval from the Johns Hopkins School of Public Health IRB as well as the relevant country research ethics committee prior to survey data collection. Verbal and written informed consent are obtained individually from all participants before the questionnaires are administered.
What will I find on this website?
Malaria Behavior Survey Toolkit
The Malaria Behavior Survey toolkit consists of a set of standard survey questionnaires (women’s, men’s, household), templates, and tools to guide implementation of the survey. New resources are added to this toolkit as they are developed.
Malaria Behavior Survey ToolkitCountry Results
Country-specific pages contain reports detailing the MBS results and include the survey tools used, as well as external links to datasets on the USAID Digital Data Library, as they become available. These pages are updated regularly.
Country Results